
One Nurse, Many Beginnings: Gilly Burn and the Early Story of Palliative Care in India
There are some people whose influence on palliative care cannot be measured solely by the institutions they build, the policies they write, or the awards they receive. Their contribution lives on quietly through the people they encouraged, the services they helped inspire, and the conversations that changed the direction of care. Gilly Burn is one such nurse. A story of nursing leadership, advocacy, courage, and the many beginnings that helped shape compassionate care.

Speaking from her seaside home in the United Kingdom, Gilly Burn reflected not only on the history of palliative care in India but also on the relationships, risks, and unexpected moments that shaped its earliest beginnings. Her memories are deeply personal, often emotional, and filled with what she repeatedly calls “serendipity”, those unplanned moments that unexpectedly change the course of life.
Although many associate the formal growth of palliative care in India with later institutional developments, Gilly’s journey began much earlier. She first visited India in 1984 and was deeply affected by what she witnessed in hospitals. “I was shocked,” she recalls simply. That experience stayed with her.
In 1988, in what she fondly calls “serendipity,” her name was drawn at random from a raffle to attend the 5th International Cancer Nursing Conference at the Royal Festival Hall in London — where she met Dr Jan Stjernswärd, then Chief of the WHO’s Cancer and Palliative Care Unit. Their meeting eventually led her to undertake a WHO-supported needs assessment for palliative care in India in 1989.
What she encountered during those early travels was both inspiring and painful. Palliative care was largely unknown. Oral morphine access was extremely limited. Nurses had little visibility in decision-making. On arrival at one hospital, she was told bluntly, “we have no place for nurses.” Yet she also encountered clinicians willing to listen, experiment, and imagine something different for patients living with serious illness.
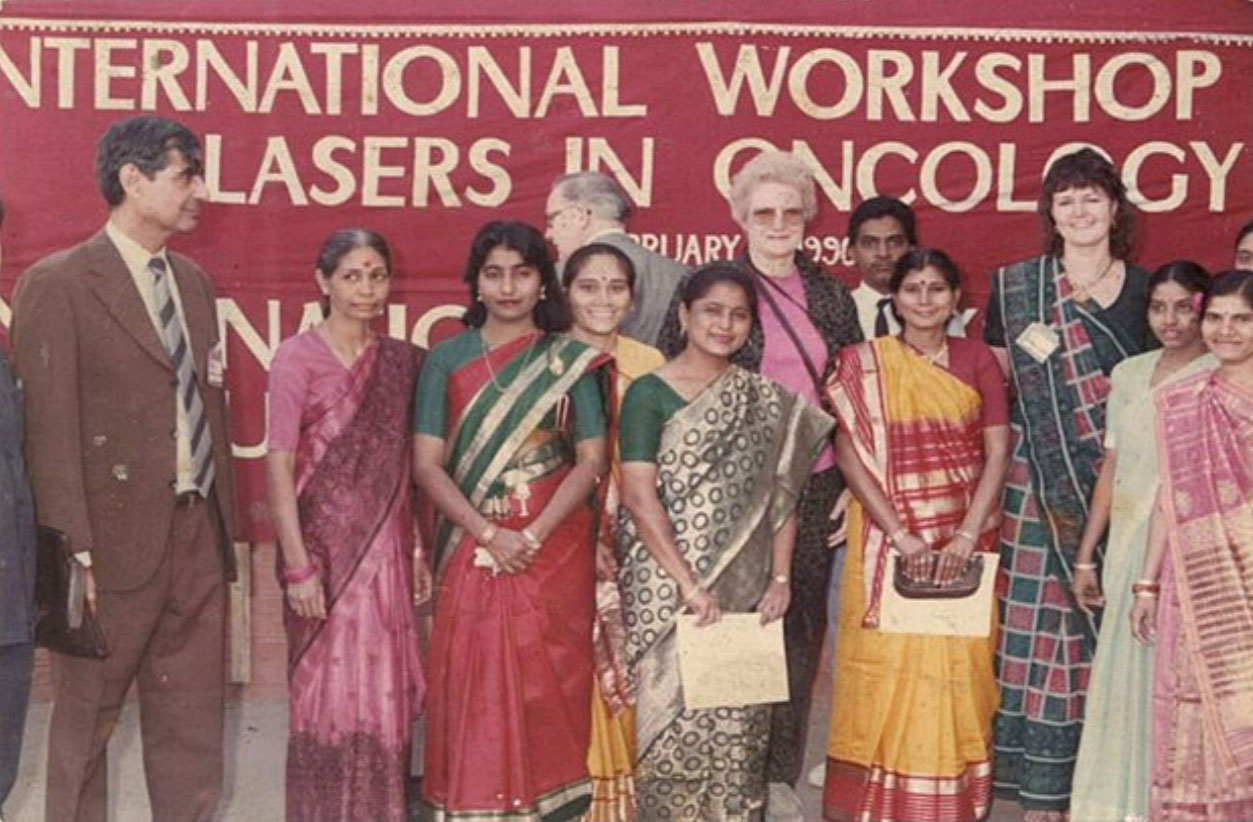
Travelling across cities including Delhi, Ahmedabad, Kerala, Mumbai, and Manipal, she carried little more than teaching materials, photographs, and conviction. Her presentations were simple, often using handwritten transparencies on overhead projectors, but the stories and images she shared moved audiences deeply.
One such moment would later become part of Indian palliative care history. During a conference in Mumbai, Gilly spoke briefly about hospice care and provided practical information on accessing oral morphine in India. Among those listening was Dr C.D. Joseph from Kerala, who later became one of the first doctors in the state to obtain oral morphine tablets for patients. For Gilly, this reflected an important truth: small moments can create lasting change. As she puts it: “I might only touch one heart, but it might be a heart that changes the world.”
Yet throughout the conversation, Gilly repeatedly returned to nurses.
“If you haven’t got a good nurse on duty, pain will never be managed,” she says firmly.
For her, nursing was never secondary to palliative care, it was central to it. She speaks passionately about the importance of bedside nurses, clinical competence, communication, and advocacy. She worries that many nurses are moved away from patients too early in their careers and believes nursing education must remain grounded in real patient care. To illustrate what she means, Gilly returns to one of her own bedside practices. Before any procedure on an unconscious or unresponsive patient, she would speak to them aloud naming herself, naming what she was about to do, and refusing to treat silence as absence.
“My name is Gilly. I know you can’t see me, but I’m here. I’m going to do your blood pressure; you’ll hear me pumping up the cuff. I’m going to move your leg; I’m going to turn you over.”
It is her philosophy of nursing in a nutshell. Presence over procedure, attention as care, and the conviction that the patient is never simply a body on a bed.

Her commitment to education became one of her most enduring contributions. Through Cancer Relief India, the charity she founded after her early visits, she supported training opportunities for Indian clinicians, including some who later became major figures in palliative care development. She also advocated strongly for nurses to receive the same educational opportunities as doctors, something uncommon at the time.
Among those she helped support was Mrs. Kumari Tankam, who in 1999 became the only nurse from India to hold the diploma in palliative nursing from Oxford Brookes University in the United Kingdom, a qualification she earned with distinction. The story behind it was itself an act of vision. Dr Krishnan Nair, the Radiation Oncologist at the Regional Cancer Centre in Trivandrum, asked Gilly to take Kumari to the UK for three months’ exposure to palliative care. Oxford regarded her so highly that Gilly was able to persuade him to let her stay a full year, so she could complete the diploma. She returned to India in 1999 with a rare and high-level qualification.
What followed, Gilly reflects with regret, was a missed opportunity. Kumari was not only an exceptional nurse but an excellent teacher; her skills, fully used, could have shaped the practice of countless thousands of patients. But the hierarchy of the time did not encourage her to share what she had learned. For Gilly, this is one of India’s enduring challenges. “We really need to encourage creativity from young and upcoming nurses,” she says.
Importantly, Gilly does not tell the story of palliative care in India as the achievement of one person or institution. Instead, she describes it as a movement built through relationships, mentorship, persistence, and collective effort. She speaks warmly of pioneers such as Dr M.R. Rajagopal, Dr Suresh Kumar, Dr Mohan Bhatia, Dr Akhileshwaran, Dr Krishnan Nair, and many nurses whose dedication and contributions helped shape the early growth of palliative care in India. She speaks with particular warmth of Dr Mohan Bhatia of Ahmedabad, whom she credits as one of the early pioneers to lay strong foundations for the growth of palliative care in India.
Among the stories she recalls most emotionally is that of the early nurses trained in Ahmedabad in 1989. She lived on the campus of the Community Oncology Centre and Hospice Complex for ten days, working alongside Dr Mohan Bhatia, and the four nurses, Vimla Ben, Rita Ben, Diraj Ben, and Gauri Ben alongside Anila Ben, the matron, recently passed away, whose memory Gilly cherishes. Decades later, she still remembers their names and believes their role in the foundation of palliative care deserves greater honour and visibility. Her engagement extended well beyond that first stay. She was part of the formation of the Indian Association of Palliative Care (IAPC) in 1994 and served on the Scientific Committee that designed the sessions for the very first IAPCON, held in Varanasi later that year. The following year, she returned as faculty for the 2nd IAPCON in Ahmedabad. In 2018, she came back once more to the same Ahmedabad hospice, nearly three decades after she had first lived on its campus.
“Hospice is a philosophy, not a building,” she often repeats — quoting Dame Cicely Saunders.
For her, the heart of palliative care lies in human relationships — in listening, teaching, accompanying those who suffer, and creating systems where dignity matters.

Even after decades of work, her reflections remain strikingly relevant today. She speaks openly about professional hierarchies, the undervaluing of nurses, and the need for greater courage within healthcare systems. Yet despite the frustrations she describes, what remains strongest is not bitterness, but hope.
She continues to believe deeply in the potential of nurses to shape the future of palliative care.
“Nurses have got something very special to offer,” she says quietly.
Asked what message she would offer this Nurses’ Day, Gilly is unwavering. Nurses who teach must continue to ‘nurse.’ “That is what has enabled me to make my teaching credible,” she says — “because I’ve maintained my clinical competence.” Her prescription is concrete: a day a week, two days a month. Professors and tutors of nursing in India, she insists, must keep a clinical component in their work. “Only then will we really start to see a change in the nursing profession.”
Perhaps that is the enduring lesson of her story. The early history of palliative care in India was not built only through policies or institutions, but through ordinary people willing to speak, teach, travel, challenge systems, and stand beside patients.
And among those many beginnings was one nurse who refused to stay silent.
Snippets from an online interview series with Gilly Burn, in conversation with Terrymize Immanuel and Anu Savio Thelly, reflecting on the early journey of palliative care development in India. A story of nursing leadership, advocacy, courage, and the many beginnings that helped shape compassionate care.